Condition treated
The most important point to remember is that everyone with a bowel problem can be helped and many can be completely cured.
It is never too late to get help with your bowel problems. If you would like some advice on how to approach your GP regarding your bowel problem do get in touch.
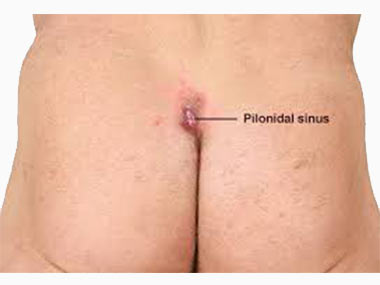
Pilonidal Disease
Pilonidal sinus is an infected tract under the skin between the buttocks. Pilonidal disease affects mostly young males and may present as asymptomatic pits, acute abscess formation, or chronic discharging sinuses. Risk factors for pilonidal disease include male gender, hirsute individuals, Caucasians, sitting occupations, existence of a deep natal cleft, and presence of hair within the natal cleft. Family history is seen in over 1/3 of patients with pilonidal disease. Obesity is a risk factor for recurrence.
Pilonidal Disease
Pilonidal sinus is an infected tract under the skin between the buttocks. Pilonidal disease affects mostly young males and may present as asymptomatic pits, acute abscess formation, or chronic discharging sinuses. Risk factors for pilonidal disease include male gender, hirsute individuals, Caucasians, sitting occupations, existence of a deep natal cleft, and presence of hair within the natal cleft. Family history is seen in over 1/3 of patients with pilonidal disease. Obesity is a risk factor for recurrence.
Presentation
The most common presentation of pilonidal disease is a painful, swollen lump in the sacral region, about 4-5 cm above the back passage. Patients may present with intermittent swelling and drainage of purulent or bloody fluid from the area. Loose hair may be seen projecting from the site.
Treatment
Pilonidal abscess
This is treated with prompt incision and drainage, in most cases under a general anaesthetic. The wound is left open and cleansed daily in the shower or with a sitz bath. In 90% of cases the wound is fully healed within a month.
Unfortunately, this is not a long-term curative procedure and as many as 85% of patients require further surgical treatment.
Pilonidal sinus
Surgical options for management of chronic pilonidal sinus include the following: