Procedures
The most important point to remember is that everyone with a bowel problem can be helped and many can be completely cured.
Whenever possible, we offer procedures using minimally invasive techniques.
Pilonidal Sinus Surgery
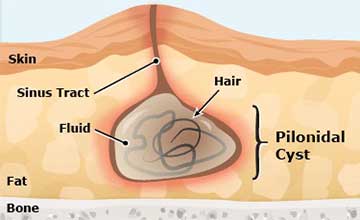
A pilonidal sinus (PNS) is a small hole or tunnel in the skin. It may fill with fluid or pus, causing the formation of a cyst or abscess. It occurs in the cleft at the top of the buttocks. A pilonidal cyst usually contains hair, dirt, and debris. It can cause severe pain and can often become infected. If it becomes infected, it may ooze pus and blood and have a foul odor.
A PNS is a condition that mostly affects men and is also common in young adults. It’s also more common in people who sit a lot, like cab drivers.
The ideal treatment of pilonidal disease varies according to the clinical presentation.
Acute Pilonidal Abscess
A pilonidal abscess is managed by incision, drainage, and curettage of the abscess cavity to remove hair nests and skin debris. The wound is left open and cleansed daily in the shower or with a sitz bath. In 90% of cases the wound is fully healed within a month. Unfortunately, this is not a long-term curative procedure and as many as 85% of patients require further surgical treatment.
Chronic Pilonidal Sinus
Conservative measures
One of the easiest interventions is to shave the sacral area free of hair and to pluck all visible embedded hair in the sinus.
Laser hair removal treatment to the region or ablation of the sinus has been proposed to decrease the likelihood of further exacerbations but has not gained popularity. Similarly, application of fibrin glue after curettage of the tract has no confirmed efficacy.
Surgical procedures
Excision and laying open of sinus tract
The pilonidal sinus is excised and the tract is laid open to allow healing by secondary intention; this technique avoids the wound infections that can be seen after primary closure. The average time for wound healing to occur is approximately 6 weeks. Application of negative pressure wound management systems (Vac therapy) might decrease healing times. The recurrence rate is in the range of 10-20%.
Excision with primary closure
Primary closure has the potential for earlier wound healing if infection does not occur; the incidence of failed primary healing is approximately 15%. Recurrence rates may be as high as 40%.
Incision and marsupialization
With marsupialization, after the pilonidal sinus is excised, the wound is sutured open and loosely packed; daily dressing changes are required. Marsupialization provides the patient with a smaller wound as compared with wounds that are left open to granulate. Healing is usually complete by 6 weeks, and the recurrence rate has been reported to be below 10%.
Bascom procedure
The Bascom procedure focuses on removal of the hairs and follicles with small wounds and a shorter healing time (usually less than 3 weeks). The disadvantages are wound infection and wound dehiscence. Recurrence rates are less than 10%.
Karydakis procedure
This uses an asymmetrical or oblique elliptical incision in an attempt to keep incisions out of the natal cleft. Once the sinus is excised, a full-thickness flap is created on the opposite side allowing it to be mobilized for primary wound closure, thus avoiding a midline wound. The wound is closed in multiple layers over a closed suction drain. Recurrence rates are typically below 5% but flap failure and wound dehiscence can be problematic.
Complex or recurrent pilonidal disease
The techniques developed for recurrent disease and unhealed wounds generally involve the use of a flap procedure to achieve primary closure and to obliterate the deep natal cleft. The procedures available include the following:
These carry the risk of flap failure and prolonged hospitalisation with the frequent use of drains.