Procedures
The most important point to remember is that everyone with a bowel problem can be helped and many can be completely cured.
Whenever possible, we offer procedures using minimally invasive techniques.
Bowel Resections
Surgery is the only curative modality for localized colon and rectal cancer (stage I-III) and potentially provides the only curative option for patients with limited metastatic disease in liver and/or lung (stage IV disease).
Indications
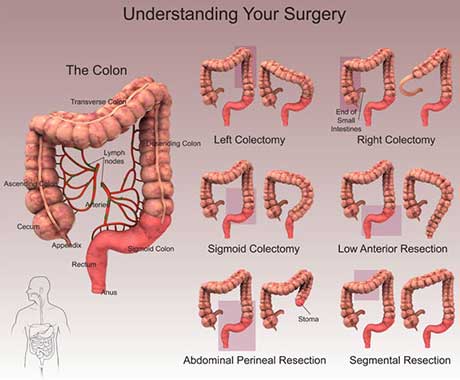
For lesions in the cecum and right colon, a right hemicolectomy is indicated. Lesions in the proximal or middle transverse colon, are generally treated by an extended right hemicolectomy. For lesions in the splenic flexure and left colon, a left hemicolectomy is indicated. For sigmoid colon lesions, a sigmoid colectomy is appropriate. Total abdominal colectomy with ileo-rectal anastomosis may be required for patients with any of the following:
Laparoscopy
The advent of laparoscopy has revolutionized the surgical approach to colonic resections for cancers. Large prospective randomized trials have found no significant differences between open and laparoscopic colectomy with regard to intraoperative or postoperative complications, perioperative mortality rates, readmission or reoperation rates, or rate of surgical wound recurrence. Oncologic outcomes (cause-specific survival, disease recurrence, number of lymph nodes harvested) are likewise comparable. However, laparoscopic surgery offers several advantages: earlier hospital discharge, return to work and normal activities, less post-operative pain, lower incidence of incisional hernias and post-operative adhesions and reduced rates of surgical site infections (SSI); the cosmetic appearances are also improved.
For rectal cancer, surgical options are:
Robotic surgery
Robotic surgery has been proposed as being able to offer better dissection and access for rectal tumours; however, it has higher costs and there is as yet no hard evidence of its superiority over conventional laparoscopic surgery.
Initial reports point towards lower rates of conversion to an open procedure, better quality of resection with preservation of pelvic nerves essential for maintaining sexual and bladder function, and lower risk of margin involvement by tumour.
